Posted on April 3, 2025
What’s New?
Share the Medicaid Petition Flyer
Medicaid Cuts Impact New Jersey, Sign Petition
Posted on March 10, 2025
Federal Budget Cuts will Pose a Financial Strain on New Jersey and Threatens Essential Healthcare Services for Children and Families
The NJ Department of Human Services has assessed how Congressional budget proposals could impact Medicaid provider pay, eligibility, and benefits—affecting thousands of children and families statewide.
Federal funds cover over half ($14B) of NJFamilyCare’s $24B budget. Cuts could jeopardize vital services, forcing families to choose between healthcare and basic needs.
The state's healthcare coverage program, NJFamilyCare, covers 1.8 million New Jerseyans- including 830,000 children and 80,000 young adults.
Who are these children?
- Children from poor to moderate income working families
- Children living in foster care
- Young people recently aged out of foster care and just entering the workforce
- Children adopted from foster care with special needs
- Children living in kinship care families
- Children receiving services through NJ's Children System of Care
- Children with developmental disabilities
- Children with complex medical and health needs
- Children receiving Medicaid school-based health services
- Children with IEPs and needing health-related services in school
Medicaid also assists adults with disabilities and seniors living in long-term care facilities.
What services are at stake?
The coverage includes life-saving care and essential services that prevent costly and invasive health problems in the future. Some of these services include:
- Hospital Care
- Physician (Primary Care and Specialty)
- Dental Care
- Prescription Drugs
- Maternal Health (This includes more than 30% of New Jersey births)
- Long-term nursing care, in nursing facilities and the community
- Behavioral health, including services for those with serious mental illness and treatment of substance use disorders
- Community-based services for individuals with developmental disabilities
ACT NOW: Tell Congress you oppose Medicaid cuts that will affect our most vulnerable citizens.
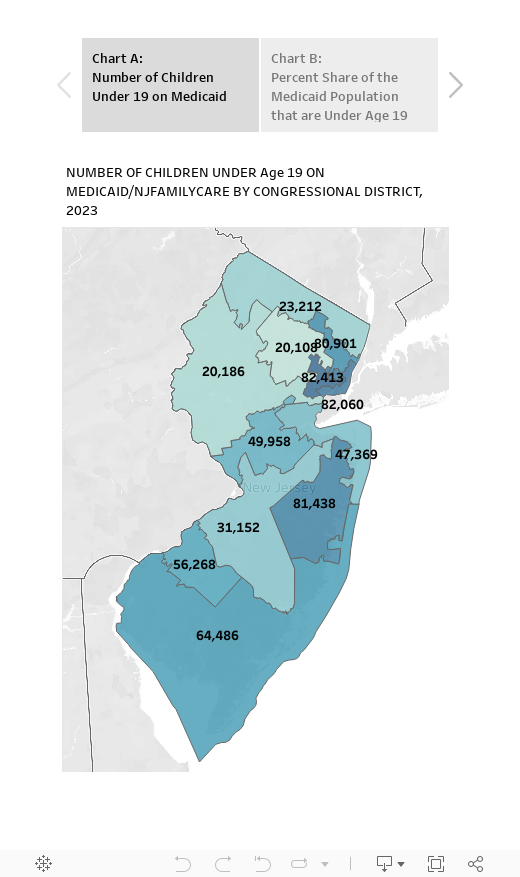
In New Jersey, 830,000 children depend on NJFamilyCare for their healthcare needs. View the chart below to see how many live in your congressional district. Map B shows that children stand to lose most because they make up the larger share of the Medicaid population.
Share on Social Media
Tell your family, friends, neighbors, and clients essential healthcare is at risk!
𝐏𝐫𝐨𝐭𝐞𝐜𝐭 𝐍𝐉’𝐬 𝐅𝐚𝐦𝐢𝐥𝐢𝐞𝐬 – 𝐒𝐭𝐨𝐩 𝐌𝐞𝐝𝐢𝐜𝐚𝐢𝐝 𝐂𝐮𝐭𝐬! 𝐒𝐭𝐚𝐧𝐝 𝐰𝐢𝐭𝐡 𝐀𝐂𝐍𝐉—𝐬𝐢𝐠𝐧 𝐭𝐡𝐞 𝐩𝐞𝐭𝐢𝐭𝐢𝐨𝐧 𝐓𝐎𝐃𝐀𝐘!
— AdvocatesforChildren (@ACNJforKids) March 13, 2025
Here is our Petition Link: https://t.co/sPV7s4NZdK#ProtectMedicaid #HealthcareForAll #NJFamilies #ActNow
ACNJ’s Testimony in Support of Bill A2291 (expanding child care assistance to all full-time child care workers)
Posted on March 10, 2025


TO:
Asw. Shama A. Haider, Chair
Asm. William W. Spearman, Vice Chair
Members of the Assembly Committee on Children, Families and Food Security
FROM: Winifred Smith-Jenkins, Ed.D, Director of Early Learning for Policy and Advocacy
Cindy Shields, Senior Policy Analyst for Early Childhood, Advocates for Children of New Jersey
DATE: March 10, 2025
RE: A2291 (categorical eligibility, expanding child care assistance to all full-time child care workers)
Good morning, Chairwoman Haider and members of the committee. Thank you for the opportunity to speak today in strong support of Assembly Bill 2291.
Child care is not just a service—it is the backbone of our economy. Right now, New Jersey’s child care system is in crisis. Providers are struggling to keep their doors open, child care workers are leaving the field due to poverty wages, and families are trapped on endless waitlists or forced to leave the workforce because they can’t find affordable early care and education. We ask these dedicated professionals to care for and educate our youngest learners, yet we pay them wages so low that many struggle to afford care for their own children. Of the nearly 26,000 child care workers in our state, only 859 currently qualify for child care assistance (a mere 3%). That means thousands of the very people we entrust with our children are forced to make impossible choices—often leaving the field altogether, worsening the workforce shortage.
When child care workers cannot afford child care, the entire economy suffers. Parents rely on child care to work, businesses depend on a stable workforce, and young children thrive when they have consistent, high-quality teachers. But right now, we are failing both our families and our workforce. High turnover in child care centers disrupts children’s learning and development, puts stress on providers, and leaves businesses struggling when employees can’t find stable care. This bill would support child care professionals and incentivize individuals to stay in the field, ensuring recruitment and retention of qualified educators.
A2291 is a common-sense solution that other states—including Kentucky, Washington, Massachusetts, and others—have already embraced. By expanding child care assistance to all full-time child care workers, begin to stabilize this critical workforce, reduce turnover, and strengthen New Jersey’s economy.
Child care is not just a service—it is the foundation of our economy. Fully funding DHS must be our highest priority because without it, our workforce crumbles. Any cuts would be catastrophic, forcing child care providers to shut their doors, driving workers out of the field, and leaving families without the care they need to stay employed. The ripple effects would be felt across every industry in New Jersey. If we are truly committed to supporting working families and building a stronger economy, we must not only protect DHS funding but expand it. Child care workers are essential to keeping our economy running—it’s time we invest in them like our future depends on it, because it does.
I urge you to pass this bill and recognize child care workers for what they are: the backbone of our workforce. Thank you for your time and consideration. Should you have any questions or need additional information, please feel free to reach me at cshields@acnj.org.
ACNJ’s Testimony in Support of Bill A4365 (establish Council for Community Recovery and Family Success)
Posted on March 10, 2025

TO:
Asw. Shama A. Haider, Chair
Asm. William W. Spearman, Vice Chair
Members of the Assembly Committee on Children, Families and Food Security
FROM: Mary E. Coogan, President & CEO, Advocates for Children of New Jersey
DATE: March 10, 2025
RE: A4365, that will establish the Council for Community Recovery and Family Success in, but not of, the Department of Community Affairs
Advocates for Children of New Jersey (ACNJ) thanks this committee for providing the opportunity to offer comments in support of A4365, that will establish the Council for Community Recovery and Family Success in, but not of, the Department of Community Affairs. The 25-member Council will develop strategies to strengthen families before they need assistance due to distress. The bill appropriates $4.0 million from the General Fund to the Council to implement the provisions of this legislation.
In order to implement the Statewide initiative, the Council will establish community recovery and family success councils in each county to develop an integrated service planning and delivery system that promotes community connections, and preventive services to ensure financial security, quality education, health, safety, and permanency for infants, children, youth, and families in that county.
ACNJ appreciates the goal of establishing community recovery and family success councils in each county based upon an assessment of need and county readiness, giving parents, community leaders, local government, and non-profit service providers the authority to identify and fund programs and services that will enrich their communities and enable families to thrive. The local service plans, designed by the county and communities they serve, and approved by the state-level Council, are a promising step towards more targeted investments that support prevention and success, ultimately improving social and economic outcomes for children and families. The assistance from the state Council through the development of community-informed family success outcomes measures and objectives will help ensure the success of the county councils.
ACNJ asks this Committee to support A4365.